Delivering High Quality Brain and Spinal Surgery
Brain Tumours
Introduction
Brain tumours often present via the emergency pathway with features of raised pressure (headache, vomiting, and drowsiness); with seizures; and as stroke mimics (focal disturbance of brain function).
Often the first test is a head CT scan. Brain MRI gives much more detail.
Tumours may also be identified on brain scans either responsible for the patient's symptoms, or part of screening or staging tests, or simply as incidental findings.
All patients should be referred to a neurosurgeon for further evaluation.

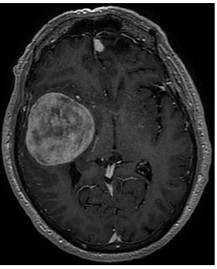
Meningioma
A benign brain tumour arising from arachnoid cap cells. These tumours are generally slow growing. Many may be observed with serial MRI scans over many years.
These tumours have characteristic features on MRI, and these may be used to predict likely growth.
Surgery is curative. Rarely radiotherapy may be needed. Gamma knife stereotactic radiosurgery can prevent growth if surgery is thought to be an excessive risk.
The IMPACT score is currently being validated. This can help to guide MRI surveillance plans.
Metastases
Commonest tumours in the brain. Unfortunately, the extent of the primary cancer limits treatment options in many cases. However, the improved responses to chemotherapy and immunotherapy mean that with longer survival more and more patients are receiving treatment for brain metastases. Often these systemic treatments are very effective for extra-cranial disease - ie good for the body, but not effective within the brain.
Characteristic features on MRI - multiple lesions with lots of associated oedema (swelling)
Primary cancers metastasising to brain

Glioma
These primary brain tumours have the highest annual incidence. Low grades (WHO grades I and II) have the potential to have curative surgery, whilst high grade tumours (WHO III and IV) need adjuvant chemoradiotherapy to improve survival. Advances in neurosurgical techniques, monitoring, and imaging can improve resection and reduce operative neurological complications.
Surgery obtains an accurate tissue diagnosis- either with a biopsy (sampling) or through a resection of the tumour. Resection can improve symptoms, improve oncological options (tolerance of radiotherapy and chemotherapy), and improve survival, but can risk neurological worsening (disability).
